
What is Kashin-Beck disease?
Kashin-Beck disease is an endemic degenerative disease of the musculoskeletal system, which is based on the primary impairment of enchondral growth of tubular bones and ossification processes. Developing then deformations of the joints with osteophytosis and without signs of inflammation give reason to consider Kashin-Beck disease as endemic deforming osteoarthritis.
The first mention of this disease belongs to M. A. Dokhturov (1839), but NI Kashin (1859) and E. V. Beck (1906) made a detailed description of it. The disease is most common in Transbaikalia, in the area of the Level river, hence its second name – Urarian disease. Later it was found that the disease occurs in other areas of Eastern Siberia in the form of separate endemic foci, as well as in China, Korea. Selected cases of the disease were noted in Primorsky Krai, Kyrgyzstan and the European part of Russia. In the foci of endemia, according to E.V. Beck, the disease was ascertained in 32% of the population, and in some villages – in 46.5%. Currently, due to the development of its treatment and prevention methods, the spread of the disease has decreased. Thus, according to LF Kravchenko, it is detected in 95.7 per 1000 inhabitants of an endemic focus.
Sick children and young men, both male and female. The disease develops only during the growth period, most often at the age of 6-14 years, when the greatest growth of the skeleton is observed. The disease is never detected in children younger than 4 years old, and after the age of 25 it develops extremely rarely.
The disease is characterized by a chronic progressive course with multiple symmetrical lesions of the joints, with the formation of pronounced deformities. The most characteristic symptoms are short stature and shortness caused by impaired bone growth in children and adolescents.
Causes of Kashin-Beck Disease
The etiology of Kashin-Beck disease is not well understood. The most reasonable is the geobiochemical (mineral) theory proposed by A. B. Vinogradov, according to which Kashin-Becke disease is the result of an unbalanced amount of calcium and trace elements in the body due to a lack of calcium and an increased content of iron, strontium, manganese in soil, water and food those areas where the disease is common. Calcium deficiency and a high content of iron, manganese, zinc and silver were found in the bone tissue of patients.
A. B. Vinogradov, V. V. Kovalevsky and V. G. Khobaryev, studying the soils in the Livski region, found that where there are limestone fields (there is a lot of calcium in the water), few patients with a disease with a disease are detected. The importance of hyposelenism, a lack of water and soil in the village, is also discussed (especially by Chinese authors).
Employees of the Chita Research Problem Research Laboratory for the Study of Uray Disease in Chita found that the imbalance of macro and microelements in endemic areas is mainly due to the elevated phosphate content in soil, water and local food. An examination of the population of these areas revealed an increase in the level of inorganic phosphorus in the blood serum and in the urine of patients with common disease. Chronic phosphorus intoxication in experimental animals caused phosphatemia, bone growth and joint changes, similar to those observed in patients with level disease. The authors of the “phosphate” hypothesis believe that as a result of excessive intake of phosphate into the body, hormonal regulation of phosphate-calcium metabolism is disturbed and hormone osteogenesis is “disrupted”.
All these observations confirm the primary role of microelements in the disruption of osteogenesis processes in disease levels. Apparently, an excess or deficiency of certain mineral salts leads to calcium deficiency in the bone tissue of the epiphyses and the development of the disease. According to LF Kravchenko, collagen metabolism is disturbed and fibrinolysis is inhibited, which contributes to microcirculation disturbance in the metaepiphyseal epiphyses, retardation of the regenerative processes of connective tissue elements, disruption of osteogenesis and early synostosis with subsequent development of degenerative changes in articular tissues and internal organs.
The role of heredity is not proven, but there is evidence to indicate the value of this factor. So, F. P. Sergievsky found that sick children are born 2 times more often than sick people in patients with a Ura disease of their parents. Yu. A. Domaev, having investigated 461 families, where there were patients with a lesion of the disease, established a higher percentage of morbidity among blood relatives than among those who are distant. The author believes that this indicates a hereditary genesis of urai disease with an incomplete manifestation of the genotype, in the realization of which a large role belongs to the environment of the endemic region.
According to many authors, rickets is a predisposing factor, since hypoavitaminosis D impairs the absorption of calcium salts and, thus, contributes to an earlier and more pronounced development of level disease. Factors conducive to the development of the disease may also be physical overload and hypothermia.
Pathological anatomy
In case of Kashin-Beck disease, there is a generalized degenerative process in the bones and joints with a significant impairment of the processes of ossification. Mainly affected are epiphyses and metaphysical long tubular bones. The process begins with dystrophic changes in the zone of preliminary calcification of the metaepiphyseal department of bone. During normal osteogenesis, in this zone, calcification occurs first, then cartilage resorption and replacement with bone tissue. With Kashin-Beck disease, both processes are violated.
The preliminary calcification zone is discharged, then thickened and hardened, and finally a gradual disappearance. Multiple grooves, grooves and holes resembling vascular appear on the articular surfaces of the bones, as a result of which the entire articular surface appears broken, porous and deformed. At the same time erosion and destruction is not observed. Characteristic are the peculiar recesses of the articular depressions in the form of a bell or niche into which parts of the epiphysis are wedged, as well as an uneven increase in the epiphysis in width.
Since all these changes are localized in the germ zone of the tubular bones and develop during the period of greatest growth of the skeleton, the normal growth of the bones is disrupted, which causes the short stature of these patients. A typical slowdown in the growth of phalanges (mainly the middle phalanx), which leads to short fouls.
In a later stage, phenomena of deforming arthrosis develop, which is facilitated by a significant change in the congruence of the articular surfaces. Fragmentation, exfoliation and destruction of the articular cartilage occur, but it can remain thickened. In these cases, seals of the subchondral bone (osteosclerosis) characteristic of osteoarthrosis are not formed. The abundant osteophytes developing in Kashin-Beck disease are not only marginal, but can also “flow” onto the articular surface, sometimes hanging over it.
Significant defiguring of the articular surfaces leads to their displacement and subluxation, to significant disfigurement of the joint and restriction of movement in it. Ankylosis is never formed. Deformities of the joints, violation of statics and improper distribution of the load contribute to the formation of muscle contractures.
In the synovial membrane, there is significant hyperplasia of the villi with their frequent separation and the formation (together with pieces of necrotic cartilage) of free intraarticular bodies (“articular mice”). Sometimes there are small phenomena of reactive synovitis. The deformation of the endplate of the vertebral bodies with recesses in them and the introduction of protrusions of intervertebral discs occurs. However, unlike the Schmorl nodes, the continuity of the plate is not broken. On some surfaces of the vertebral bodies there are bony protrusions with their introduction into the disks. The height of the disks can be either increased, then reduced. Discs may be bent. Significant osteophytes and sometimes calcification of the anterior longitudinal ligament are formed along the edges of the vertebrae.
Microscopically, necrotic patches are found in the main substance of cartilage – reducing the number of proteoglycans, unmasking collagen fibers, collagen fibrils collapse. In the middle zone, one can observe the proliferation of chondrocytes. The restructuring of the bone structures dramatically inhibited. In long bones, growth arrest lines are observed, indicating periodic interruptions in bone growth.
Symptoms of Kashin-Beck Disease
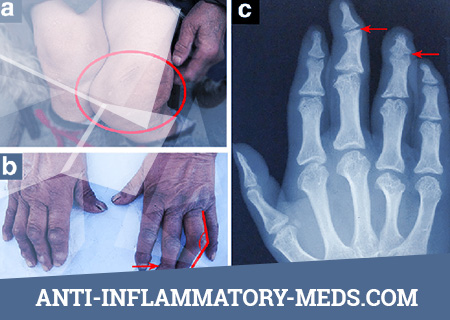
The disease develops slowly and imperceptibly in children and adolescents. The first manifestations of the disease are intermittent, aching pains in the joints, in muscles, in the spine, stiffness and crunching in the vessels, paresthesias and cramps in the fingers and in the calf muscles. First of all, II-IV interphalangeal joints of the hands are affected, and in some cases this process stops. However, progression of the disease with lesions of the wrist, elbow and all other joints is more often observed. The lesion of the joints is multiple and symmetrical with the gradual development in them of thickenings, deformities, limitation of mobility and small muscular atrophy. Often there is a curvature of the axes of the limbs and fingers. The pains in the joints are aching, non-permanent, very moderately expressed, often in the evenings and at night, they may appear much later than the development of deformity. When an “articular mouse” is impaired, a syndrome of “blockade of the joint” arises – a sharp pain, impossibility of movement and rapid swelling, most often in the knee joint.
There are three severity of the disease.
- Moderate thickening of the proximal interphalangeal joints of the II, III, IV fingers of the hands, pain under load, slight restriction of movements in the wrist, elbow and ankle joints.
- Multiple lesions of the joints with their thickening, deformation, crunch and restriction of movements. Muscle atrophy and muscle contracture. Low height (for men, 160.2 ± 0.6, for women, 146 ± 0.5). Korotkopalost.
- All joints are deformed and thickened. Movement in them is sharply limited. Short stature (160.2 ± 0.6 in men, 144 ± 0.5 in women), short neck, bear paw, genu valgum and genu varum, flat-footed, lumbar hyperlordosis, duck gait. Women often have a narrow pelvis.
In addition to these changes, neurodystrophic disorders such as headaches, heart pain, poor appetite, wrinkled skin, dull nails and hair can be observed in case of Kashin-Beck’s disease of II and III severity. Chronic atrophic rhinitis, pharyngitis, otitis media, bronchitis, pulmonary emphysema, gastritis, enterocolitis, vegetative-vascular dystonia, myocardiodystrophy, deformation of teeth and jaws, neurological disorders (asthenoneurotic syndrome, encephalopathy) are often observed. Decreased mental capacity as the disease progresses. It should be noted that if the Kashin-Beck disease develops in adults, its clinical picture may be erased. Body temperature in patients is usually normal. In the blood and urine tests are not detected pathological abnormalities. Sometimes hypochromic anemia, small lymphocytosis, and neutropenia are noted.
The study of the mineral composition of the blood shows that the calcium content is increased, and phosphorus is reduced. In urine opposite changes are noted.
Diagnosis of Kashin-Beck disease
X-ray picture
In Kashin-Beck disease, pathological signs on radiographs may be more pronounced than changes in the joints when viewed. Symmetric changes in the hands usually occur first. According to the data of D. G. Rokhlin and F. P. Sergievsky, the earliest signs of the disease are detected in the metaepiphyseal zones, where bone growth occurs in length. First, there appears a discharge of the “preliminary calcification” zone of the metaphysis, its vagueness and uneven thickening. The zone looks like a “sclerotic half moon”. Later this zone disappears, a deep impression (niche) forms in the metaphysis where the epiphysis sinks. At the same time in the epiphysis may form a protrusion, which is included in the metaphysis niche. Then comes the thickening of the metaphysis and the premature bone fusion of the metaphysis and pineal gland. On the articular surface of the epiphysis, superficial destruction with depression is observed, aseptic necrosis with subsequent thickening of the pineal gland and the development of phenomena of deforming arthrosis. However, the joint gap can be expanded due to the formation of a niche and thickening of the cartilage. In the cartilage, islands of ossification can be detected, which sometimes creates a partial double contour of the articular surface.
Multiple cartilaginous nodes (Schmorl’s hernia) and “bottle-shaped” deformation of the vertebral bodies are formed in the spinal column, and signs of deforming spondylosis are seen.
Differential diagnosis
The following symptoms are characteristic of Kashin-Beck disease, which allow to make a diagnosis: pain and a loud crunch in the joints during movement, deformation and thickening of the joints, cessation of bone growth in length with irregular proportions, short bones, short stature, joint contracture, lumbar hyperlordosis, presence on the roentgenogram pathological deepening (niche) in bone metaphysis, mainly in the hands. Of great importance are the anamnestic information about living in an endemic area.
However, since changes in the metaepiphyseal divisions occur in all diseases that cause growth inhibition in length (for example, in rickets, endocrine diseases), Kashin-Beck’s disease must be differentiated from these pathological processes. It should be borne in mind that rickets develops in children in the first years of life and already disappears by the age of 4-5, when UCLIC disease usually occurs. “Niches” with rickets develop in the long bones of the extremities, whereas in urol disease, primarily in the bones of the hands. When endocrine disorders with growth inhibition “niche” on the radiograph is not as deep as in Kashin-Beck disease, in addition, there are other endocrine disorders. With chondrodystrophy, which also develops during childhood and has many common symptoms with levity (short growth, shortening of tubular bones, deformity of epiphyses and metaphysis with their premature adhesion, hyperlordosis, duck gait), large joints are more often affected: hip, knee and shoulder. rarely joints of the hands and feet. In addition, chondrodystrophy usually begins at birth, and Kashin-Beck disease after 4-5 years. When chondrodystrophy growth is observed, movement in the joints is free, there is no crunch, deforming osteoarthritis occurs late. Chondrodystrophy is characterized by symptoms such as shortening of the base of the skull and retraction of the nose bridge, which are absent in urovskaya disease.
Acromegaly also shows thickening of the epiphyses and cartilage, flattening and protrusions on the articular surfaces, and bone growth in thickness. However, along with this, the characteristic symptoms of the disease are revealed – a thickening of the soft tissues and a change in the skull (hyperostosis of the vault, prominence of the brow ridges, an increase in the Turkish saddle on the roentgenogram), which should be taken into account when making a differential diagnosis.
Osteoarthritis gives multiple deformities of the joints, however, it develops in middle and old age, and patients do not have such characteristic signs of disease level as shortness, shortness, contractures, and the presence of a “niche” on the roentgenogram.
Treatment of Kashin-Bek’s Disease
The treatment of Kashin-Beck disease is aimed at improving the function of the joints, increasing the ability to work, reducing pain and muscle contractures. With timely and persistent treatment in the early stage of the disease in 30% of patients, according to L.F. Kravchenko et al., It is possible to achieve complete reversibility of the process, and in later ones it is possible to reduce pain, improve joint mobility and slow the progression of the process. This is achieved by using calcium and phosphorus drugs (phosphene, calcium gluconate, calcium lactic acid – 2-3 tablets per day, etc.), vitamins C, B1, Bia, as well as the means used for arthrosis – biological stimulants (aloe, vitreous body, ATP, PhiBs) in combination with the methods of physiological balneotherapy, medical gymnastics and massage. Due to the absence of pronounced pain syndrome, rare and rapidly passing inflammatory phenomena in the joints, these patients usually do not need the appointment of painkillers and anti-inflammatory drugs. The effect of radon baths (3-6 courses) in combination with paraffin and mud applications on the joints is very effective. Drops, diathermy, ultrasound and UHF for joints are also used. Treatment with radon baths in the Yamkun resort, located in the center of one of the endemic areas of Eastern Siberia, allows for an improvement, according to FP Sergievsky, in 80% of patients.
After 2-3 courses of radon baths (18–30 procedures with a water temperature of 36–40 ° C) LF Kravchenko observed not only a decrease, but a disappearance of the “niches” on the radiograph.
In the late stage of the disease, with pronounced irreversible changes in the joints, orthopedic surgery is recommended to eliminate contractures and restore movement, and with repeated blockades of the joint, the removal of articular “niche” is recommended.
Prevention of Kashin-Bek’s Disease
Prevention of Kashin-Beck disease is to eliminate the lack of calcium in water and soil in endemic areas, where. soil mineralization is being carried out; special livestock state farms are being created with mineral feeding of animals, supplying the population with imported products and water from artesian wells. Children, adolescents, pregnant and lactating women receive calcium supplements and vitamins 2 times a year. Medical observation of the physical development of children and adolescents with their referral to local resorts in case of suspected development of the disease has been strengthened. In order to prevent the progression of the disease, patients are resettled from an endemic area, which has a beneficial effect on the course of the disease.